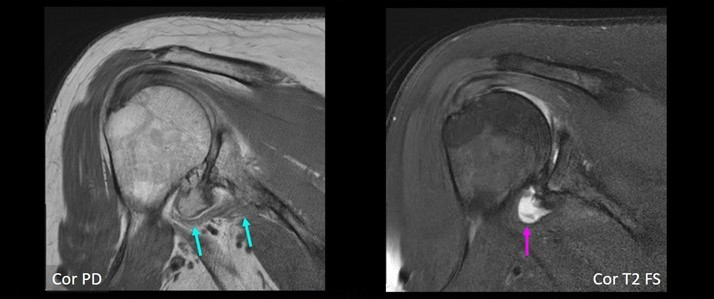
66-year-old female with severe shoulder pain. Coronal MR images show definite small AIGM (blue arrows), corresponding to diagnostic confidence of 4. In addition, there is high-grade glenohumeral osteoarthrosis, as well as small joint effusion (purple arrow).
May 7, 2024 — The Magna Cum Laude Award-Winning Online Poster presented during the 124th ARRS Annual Meeting showed a high prevalence (89%) of accessory infraglenoid muscle (AIGM) in patients with teres minor fatty infiltration (TMFI)—compared to those without (30%). Additionally, within the TMFI cohort, many AIGM abutted the axillary nerve with concomitant axillary neuropathy.
“These results stress the importance of looking for AIGM in the setting of TMFI, as TMFI on preoperative MRI has been associated with poor postsurgical outcomes,” said Jennifer Padwal, MD, from Stanford University Medical Center in California. “And the presence of AIGM on shoulder MRI could negate the need for additional imaging to evaluate the cause of TMFI.”
Padwal et al.’s institutional review of all shoulder MRIs yielded 100 patients with documented TMFI (76 men, 24 women; mean age, 58.6 years). For comparison, a respective sample of 100 shoulder MRIs in patients without TMFI (53 men, 47 women; mean age, 56.4 years) was obtained. All scans were consensus evaluated by two radiologists (one musculoskeletal attending with 25 years of experience, as well as a 4th-year radiology resident) for an AIGM with diagnostic confidence, noting muscle origin and insertion. In patients with TMFI, the distance between the AIGM and axillary nerve was measured, documenting any abnormal axillary nerve signal. TMFI was then graded via Goutallier classification, while the presence of atrophy and/or edema was noted.
Ultimately, in the ARRS Annual Meeting Magna Cum Laude Online Poster, TMFI was grade 1 in 33%, grade 2 in 32%, grade 3 in 13%, and grade 4 in 14%, with intramuscular edema in 33 and atrophy in 21 patients. AIGM was seen in 89/100 patients with TMFI; 30/100 patients without TMFI. In all cases, the AIGM originated from the inferior glenoid neck and inserted onto the humeral neck/proximal humeral diaphysis. The inferior margin of the AIGM in patients with TMFI touched the axillary nerve in 39 (46%), with abnormal signal in 23 (27%) patients.
For more information: www.arrs.org

 August 06, 2024
August 06, 2024 







