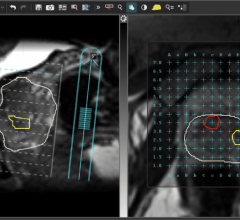
May 27, 2014 — ECRI Institute released a Health Technology Forecast regarding the use of integrated magnetic resonance imaging (MRI) to better target radiation therapy. Use of image-guided radiation therapy (IGRT) and treatment planning technology is gaining interest among clinicians who wish to increase the accuracy and precision of radiation therapy (RT). Systems that integrate a MRI scanner and RT gantry are considered a novel approach to IGRT, allowing clinicians to use both functions concurrently to guide RT with real-time images. Clinicians can reportedly use accompanying software to speed calculations for real-time adjustments to dosing, contouring and timing. Patients with tumors likely to move, or tumors located in close proximity to organs likely to move, during treatment are the most likely candidates for real-time MRI adaptive radiation therapy (ART). Use of real-time MRI ART will likely be limited until data are published that support the approach’s superior efficacy and improved patient outcomes compared with other IGRT options.
Available alternative technologies can offer near real-time or repeated interfraction ART guidance using other imaging technology; therefore, competition with these similar methodologies will likely limit use of real-time MRI ART. However, some patients and clinicians might prefer MRI guidance because it purportedly provides better soft-tissue contrast and does not expose patients to additional radiation compared with computed tomography (CT)-based image guidance.
The ViewRay system (ViewRay Inc.), which combines MRI with cobalt-60 (60Co) RT, was cleared for marketing by the U.S. Food and Drug Administration (FDA) in May 2012. As of December 2013, three facilities had installed ViewRay systems and were conducting internal studies on the efficacy of real-time MRI ART; however, none of the facilities had yet been approved by the U.S. Nuclear Regulatory Commission (NRC) to use the ViewRay for clinical applications. FDA did not require ViewRay to conduct clinical trials before marketing clearance, so limited data are available to assess its safety and efficacy. Adoption would likely increase if facilities conducting internal studies can show increased efficacy for the ViewRay system compared with other available image-guidance systems (i.e., CT-based technologies). Other real-time MRI ART systems are still in development; these are unlikely to be commercially available for clinical use before 2017.
Published data indicating that real-time MRI ART improves patient outcomes compared with available IGRT technologies are lacking. It is unclear whether movement of tumors or organs during treatment is significant enough to require real-time MRI ART, or if this approach is an improvement over other IGRT technology. Real-time MRI ART might improve health outcomes if it is proven to increase targeting accuracy, decrease radiation exposure of surrounding healthy tissues, or allows clinicians to escalate radiation doses due to increased confidence.
The ViewRay system costs about $8.5 million, with vault construction to house the system potentially costing an additional $1.5 million. If demand for this therapy increases, treatment centers could potentially recoup acquisition costs since patients receiving IGRT represent a large potential patient pool. However, as of December 2013, no ViewRay systems have been approved by NRC for clinical use and treatment pricing has not been established.
Reimbursement for real-time MRI ART from the U.S. Centers for Medicare & Medicaid Services (CMS) and private payers is not available.
For more information: www.ecri.org

 August 09, 2024
August 09, 2024