Frank Rybicki, M.D. is the director of cardiac CT and vascular CT, MRI, Brigham and Womens Hospital
Frank Rybicki, M.D., director of cardiac CT and vascular CT, MRI, Brigham and Women’s Hospital, sat down with Imaging Technology News (ITN) to talk about the Toshiba-sponsored Core-320 trial that will compare coronary CT angiography with myocardial perfusion performed on Toshiba’s Acquilion ONE against traditional invasive angiography and SPECT. The trial is set to begin later this year.
ITN: What are the clinical questions that you hope Core 320 will answer?
Dr. Rybicki: Core 320 is designed to evaluate CT in a new way. CT, in the heart, gives morphology data...anatomy and coronary imaging. It has pretty good spatial resolution and pretty good temporal resolution, and of course, it's noninvasive. In many cases at the end of the CT scan, there are still several unanswered questions. The major hypothesis of Core 320 is that the perfusion data provides added information to morphology.
ITN: Do you have an expectation going into the Core 320 on how CT will perfusion will stack up against SPECT and catheter angiography?
Dr. Rybicki: Everyone that is involved in this has high expectations. Everyone in the community is pulling for a CT system, like a wide area detector system, to do good functional imaging and do good perfusion. rk. Having all those expectations is wonderful, but you really have to roll up your sleeves in terms of proving it. You can do all you want in a small, single-center study, but the proof will be in a multi-centered and multi-national evalution.
ITN: You’ve had experience with the Aquilion ONE. Most clinicians are impressed with the spatial and temporal resolution. What has been your experience with the perfusion component?
Dr. Rybicki: The perfusion component is still in evaluation. The perfusion images I've seen to date are very good technical quality, but perfusion CT is still not a clinical tool. It has to be emphasized that using any scanner, including the
Aquilion ONE for perfusion and relying on the presence or absence of a perfusion
abnormality is in the realm of clinical research . The AquilionONE makes great
morpholic images, gives good radiation levels and it can be a used for wide
variety of things. We suspect there are good things to come.
ITN: What still needs to be worked on or corrected with CT perfusion?
Dr. Rybicki: It is hard to say because CT is so new and both modalities are attacking perfusion from different angles. In SPECT, we introduce a radioisotope that goes to the heart, then radiation is emitted from the heart out and detected by a detector system. CT is totally different. You're putting the radiation outside
through and then detecting on a system.
ITN: With CTA vs. catheter angiography, you measure the positive and negative predictive values. How do you measure CT perfusion’s performance versus SPECT?
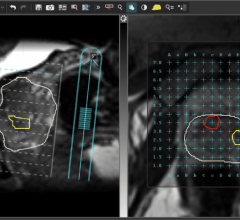
Dr. Rybicki: One way it to partition the heart muscle CT and SPECT images into segments, and then analyze each on a segment-by-segment basis. There is also a so called "bullseye" or polar map to do this kind of image analysis. These maps are also used by some imagers for diagnoses
Patients with severe disease can be managed with catheter-based intervention or surgery. SPECT is currently a key tool to separate patients. Perfusion is one piece of the puzzle used to make that distinction. If perfusion imaging, SPECT and perhaps CT in the future, suggests that there is significant myocardium that poorly perfused by viable, this is very valuable information for revascularization management. On the flip side, if the patient has a large perfusion deficit and all the tissue is dead, a large, expensive, and potentailly dangerous surgical intervention is not needed. For quite some time people have been searching for one modality that can perform these functions, and we hope that 320-detector row CT is a large incremental step in this direction.
ITN: If CT with perfusion performs well in this trial, could it be expanded to target a greater patient population rather than just low- to medium- risk patients?
Dr. Rybicki: It's unlikely that one test can do everything for all patients. Any vendor would like to be able to cover a great number of the patient population. The coronary CT part is still going to be limited by calcium. That's not going to go away with the 320. I suspect that [CT with perfusion] will still be suited for low and intermediate risk patients.
ITN: Even with the 320, heavily calcified arteries still present imaging problems for CT?
Dr. Rybicki: Absolutely. That's not going to change. One thing that would be really nice is that if you have an artery that is calcifed with multiple low-grade lesions, having a normal perfusion CT, if it were to validate that, would be very useful.

 August 09, 2024
August 09, 2024