The majority of U.S.-based healthcare facilities are either considering or implementing the consolidation of their medical image archiving in the form of a vendor neutral archive (VNA). Early experiences have taught that it is not trivial to select the right VNA, and have revealed several pitfalls during the implementation phase.
Implementing for the Right Reason
Make sure you implement a VNA for the right reason. In other words, you should have a good idea of why you want a VNA to start with.
The initial motivation for VNA purchases was in most cases to eliminate the “pain” of having to migrate images every time one changes PACS vendors, which can be costly, labor-intensive and time-consuming, often taking more than a year to get them all moved to the new PACS system. Over the past several years, the migration argument has become less important as other benefits emerged, in particular the capability of having patient-centric access to images, i.e., getting the complete set of studies, independent of whether or not a different specialty or department produced them.
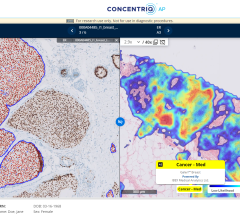
An additional advantage of a VNA is that it provides a convenient “gateway” for a universal viewer, often integrated with an EMR. A physician can review the patient history and reports, and simply click on an icon if there is an image available, and it will show up in the EMR portal. The VNA is also ideally suited to serving multiple institutions needing to share and access images on an enterprise level.
Use the Right Approach
There are two different approaches for implementing a VNA. The first one is top-down, i.e., one installs the VNA hardware and software, which could be from a vendor other than your current PACS vendor(s), and connect the various image sources. The second approach is bottom-up, by expanding an existing PACS archive and adding the functionality to make it into a VNA.
The approach often depends on the scope or range of the image archive consolidation. Five different VNA classifications can help determine the correct strategy.
Departmental VNA. This is the scenario when there is only a single department feeding the images into the VNA. The images and other objects (reports, documents, JPEGs, possibly waveforms) are all in a DICOM format and the main reason for implementing a VNA would be its “neutrality,” i.e., to facilitate future migrations and possibly to function as a portal to an EMR. An important feature is the automated synchronization of any changes that occur in the PACS and its subsequent changes in the VNA.
Multi-departmental VNA. In this case, there could be multiple departments feeding the VNA. The VNA must ensure that key identifiers are cross-referenced or made unique by adding prefixes to indicate their source — in particular non-unique accession number and patient identifiers.
Multi-specialty VNA. The difference between this implementation and the multi-departmental version is that specialties such as ophthalmology, dermatology, endoscopy and others have different workflows (encounter-based vs. order-based) and often deal with non-DICOM objects such as PDFs, JPEGs, video clips, etc. The latter means that there is a need to support the XDS protocol for data submission and retrieval.
Enterprise VNA. In this case, the VNA covers multiple sites, e.g. 1-15, which is typical for covering a metropolitan area by a small-scale IDN, a province in Canada or region in the U.K., or a Veteran’s Integrated Service Network (VISN) by the U.S. Veteran’s Affairs (VA). In this scenario, tag morphing becomes essential, and if the architecture includes a HIE, the VNA should support XDS and supporting PIX/PDQ profiles defined by IHE.
Corporate VNA. In this case, all of the images from a major healthcare consortium such as Kaiser, HCA, Tenet and others are consolidated in a central location. One could consider this as having one’s own “cloud solution.” High availability, scalability and redundancy are required features. Security is also critical, as there is a higher risk for hacking resulting from many more potential data access points. One consortium is actually starting to encrypt all data on their VNA because of the increased security exposure.
For a departmental, multi-departmental and specialty use case, a bottom-up approach might be feasible, i.e. slowly adding more features. For the enterprise and corporate VNA implementations, a top-down strategy is more effective.
Due Diligence
Implementing a VNA is not for the fainthearted, especially if one takes a top-down approach and is implementing a fully featured VNA, which transcends more than one department. The standards supporting the VNA are still emerging, notably the IOCM profile for synchronization, encounter-based workflow, XDS-I, HL7 and DICOM web services. However, one should not let this discourage or delay a VNA implementation. Simply be aware of the potential pitfalls, and make sure to select the right vendor as your partner on this journey.
Herman Oosterwijk is president of OTech Inc., and is a healthcare imaging and IT trainer/consultant specializing in PACS, DICOM and HL7. He authored this article on behalf of Novarad Corporation, in order to promote awareness and knowledge of Enterprise Imaging.

 July 26, 2024
July 26, 2024