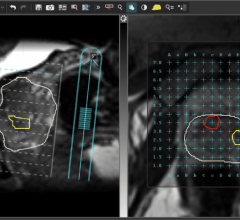
CTA of right coronary artery shows multiple sites of calcification, but no stenotic plaques.
The importance of dealing with the epidemic of coronary artery disease (CAD) is well known, and the tools at our disposal to accurately recognize and manage it are evolving in very positive ways.
Two important diagnostic tools, computed tomography (CT) and magnetic resonance imaging (MRI), play critical roles in the evaluation of coronary artery atherosclerosis. These modalities enable clinicians to perform noninvasive diagnostic tests, using coronary CT angiography (CTA) and magnetic resonance angiography (MRA), which reduce patient trauma and lower healthcare costs.
However, resistance to adopting the noninvasive approach to diagnosing CAD coupled with today’s challenging economy, threaten to hamper progress in advancing this technology and its clinical applications.
Valuable Diagnostics
Since the 1960s, we have relied on direct coronary angiography for visualizing coronary disease and directing care. There are pros and cons, and while the procedure is safe, because it is invasive, it is stressful for patients and expensive. Many feel that despite its proven value, patients are on a slippery slope toward an intervention, and often (perhaps 40 percent of the time), significant stenoses are not found, the result of false positive pre-angiographic testing. Until recently, tools to reveal the location, extent and stability of coronary plaques have been invasive: angiography and intravascular ultrasound.
However, over the past decade, the hope has grown that magnetic resonance angiography (MRA) and computed X-ray tomography (CT) may be noninvasive replacements in plaque discovery both in clinical situations, such as outpatient chest pain evaluation, or in screening applications for preclinical recognition of atherosclerosis. The results could mean better care by more accurate diagnosis and cost savings to healthcare.
But there are other issues. Despite the progress in profiling patients for clinical risk, a persisting reality is that more than half the time the disease is discovered as an emergency. Furthermore, more than half of the people presenting to our emergency rooms with acute coronary syndromes wouldn’t have even qualified for medications aimed at primary prevention the day before. And, we know that most culprit plaques in acute coronary syndromes are not stenotic plaques. If this seems complicated, that is because it is complicated.
And lastly, the world of imaging is not free of bias, and the flow of health care dollars has greatly influenced changes in “conventional” or “perceived” medical wisdom. Headlines in the lay and even in peer-reviewed journals can jolt us all to an excited state about something new and important. Learning a new vocabulary with terms such as “spiral,” “gated,” “T1 weighted,” “phase encoded,” and “dose modulated,” as well as understanding statistics is essential. The list is nearly endless, and it is confusing. Let’s try to clarify some of this here.
The Science Behind CTA and MRA
CT angiography (CTA) is an X-radiation study, which utilizes an iodinated intravenous contrast agent to change the radiation absorptive properties of coronary arterial blood and cardiac muscle. Despite the small caliber and continuous motion of the arteries, technology now allows these vessels to be resolved, successfully creating images, which are actually maps (“slices”) of contrasting tissue attenuation properties.
Magnetic resonance angiography (MRA) is usually done without an intravenous contrast agent. It relies on the magnetic properties and quantum spin characteristics of hydrogen protons (mainly in water). The heart and its blood supply are positioned in-center bore of the magnet and its trillions and trillions of hydrogen nuclei align in a very intense magnetic field. They are then pulsed with radiofrequency energy: the return of that energy is used to create a radiofrequency map, which is a high contrast soft tissue image “slice.”
By either technique, the images are slices through the heart, where the picture elements have been created through a complex flow of computer processing. The image slices have 3D properties that determine spatial resolution (CT better than MR), and contrast sensitivities that allow tissue characterization (MR better than CT). And as with all imagery, both tools are subject to artifacts that limit information content. Plus, these images come at a high time and high operational overhead. Also both tools are suited best in elective clinical situations where the pretest probability of a significant finding is intermediate. So let’s explore the differences and indications for each type of coronary artery imaging.
Clearer View of CTA
The best way to explore the differences and indications for each type of coronary artery imaging is in real-life practice, as opposed to research situations.
There are probably no metropolitan areas in the United States today that do not have a 64-slice CT scanner. For the last five years, 64-slice CT has been the workhorse scanner for high-resolution X-ray derived slices through the heart. There are four excellent competing manufacturers: GE, Philips, Siemens and Toshiba. There have been large trials revealing a high degree of accuracy to detect stenotic coronary artery segments and quantify plaque bulk in populations where cardiac catheterization has been clinically indicated.
There have also been outcome studies showing that CTA in the low and intermediate risk groups in an emergency department is a safe and efficacious triage tool. But this is at the cost of ionizing radiation, intravenous contrast material, the need for heart rate control both in rate and regularity, and particular image difficulty with high amounts of coronary artery calcium. Add to these issues reimbursement uncertainty and serious “turf” wars between the imaging specialties, and a state of confusion of what to do ensues.
The major selling point and the leading advantage of CTA over MRA is the spatial resolution. Ordinary scanners quickly acquire 0.5 mm on any plane resolution images during about a 15 second breath-held trip through the bore of the CT scanner. That is to say that the tissue volumes represented on each image, viewed in any plane of obliquity is 0.5 x 0.5 x 0.5 mm. This is sufficient resolution to study all important segments of the coronary arteries. Under ideal circumstances, plaque with and without calcium can be quantified as none, mild, moderate and severe.
The best utilization of cardiac CTA is in situations when little to no coronary disease is expected and the cardiac workup can be cut short. Therefore, patients characterized low to intermediate risk by their clinical circumstances do have clear cut indications for CTA. In the emergency department, in patients with negative cardiac enzymes and a normal EKG, a normal or nearly normal CTA can effectively rule out significant stenosis due to its high, virtually 100 percent negative predictive value. This can obviate the need for further studies, particularly invasive angiography.
In the outpatient setting, with acute and chronic chest pain cases – again with low to intermediate risk – CTA can be chosen, particularly with inconclusive stress testing data or if the patient is unable to exercise. CTA may be elected as an alternative to stress testing with or without perfusion information. The information is entirely structural and not functional, however, a negative high quality scan can end the cardiac aspect of chest pain workup.
The use of CTA as a screening test in asymptomatic individuals is not officially endorsed. However, since we know that most acute coronary syndromes occur in asymptomatic people with low to intermediate risk, an obvious conundrum exists. If the scan quality were good, the cost low and the radiation dose under 3 mSv, the public’s objections to CTA screening of intermediate risk patients, say with a worrisome family history, would be lessened.
What about CTA for patients with stents or who have had coronary artery bypass graft (CABG)? While there is literature on the high sensitivity of detecting in-stent restenosis and saphenous vein graft patency, most active centers find this a more challenging application of CTA, largely owing to the prevalence of metallic artifact, which reduces the diagnostic accuracy of the test and the generally reduced size of the target native coronary arteries. There is limited value in studying these patients with CTA.
Useful Yet Cumbersome
In CT we speak of acquisition protocols. In MR we speak of imaging sequences. Understanding the principles of physics and quantum theory that underlies this amazing technology is in a word: daunting. However, it is necessary in order to understand the proper MR sequence to answer the clinical question.
Furthermore, MRA exams are time consuming to complete – perhaps one to two hours. The imagery is hugely desirable and characterizes cardiac structure, myocardial viability, vasodilator stress perfusion, and dobutamine stress wall motion. However, in reality, a very expensive machine is tied up for a long time with each patient; this makes the case for routine use of MR angiography for atherosclerosis study in the coronary arteries difficult.
That said, there are clinical situations where coronary anatomic information without radiation exposure is the driving priority: particularly in the young population. Cardiac MRA is indicated to diagnose suspected coronary artery anomolies. The reduced spatial resolution of MRA compared to CTA is not an issue with a well-performed study. The study can be done without intravenous contrast and the signal difference between blood and surrounding soft tissue can identify the coronary origins and proximal right and left arterial segments well, in fact, better than is achievable with direct catheterization.
Kawasaki’s Disease is a vasculitis of early childhood, which can cause coronary aneurysms or frank occlusions. Here is an excellent role for MRA of the coronaries as an initial study and one that can be repeated serially without ionizing radiation. In the general adult population, left main or three-vessel coronary disease can be detected successfully, but with a lower accuracy than compared to CTA, at least in published studies so far.
Balancing Diagnostic Value With Cost
So where does this leave us in the quest to offer imaging services that have proven value, yet need to accommodate the business realities of cost cutting by third parties and the government?
The horizon holds great promise for both modalities to yield better images and, therefore, better clinical decisions. Newer, and more expensive, scanners and magnets are arriving from the leading four CT and MR vendors.
In CT, they allow shorter scan times with more rotating detector channels (currently 320 is the leader). Most importantly, a step and shoot protocol of “prospective” gating results in dramatic dose reduction to below 2.5 mSv, which everyone is exposed to in one year of living at sea level. Less widely available, but emerging refinements on MSCT (multislice CT) technology, include dual source (two X-ray sources on the rotating gantry) and the potential for two energies to separate actual plaque characteristics.
In MR, the arrival of 3.0T magnetic field strength imaging will provide better signal and contrast values in cardiac imaging. Newer support hardware and software for imaging processing will allow coronary flow measurements and hopefully plaque characterization. Examination times will decrease as better imaging sequences are developed.
However, capital budgets are tight. This means most of the American public will be served by the current modality iterations (64-slice CTA and 1.5 Tesla MRA). CTAs role will be for strictly anatomic coronary information; MRA’s role will be for function, perfusion and viability. Down the line, we can anticipate lower radiation and perfusion information from CTA, and better spatial resolution and plaque characterization from MRA.
Neither modality is going away, but for now the business will go to those enterprises that push for efficiencies in utilization: streamlined referrals, streamlined workflow, efficient use of PACS and DICOM network management, outsourced image preparation, and “read/report from anywhere” solutions.
It is a difficult time for both modalities, but echo and nuclear imaging services are facing the same economic pressures. We should pause and take a breath to see how new regulations and tighter reimbursement will affect us all.



 August 09, 2024
August 09, 2024