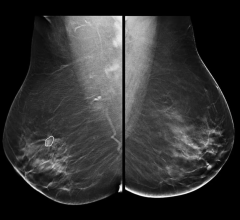
MultiHance and OMNISCAN are commonly used magnetic resonance imaging (MRI) contrast agents. Photo courtesy of Bracco.
Over the past year, headlines across industry and consumer media have highlighted FDA warnings on the dangers of gadolinium-based contrast agents. To date, it has become common knowledge and a FDA black box warning that gadolinium-based agents run the risk of causing Nephrogenic Systemic Fibrosis or Nephrogenic Fibrosing Dermopathy (NSF/NFD).
While the dust has yet not settled, the industry has turned its attention to a recent study comparing gadolinium-based contrast agents, now stirring up debate over the significance of reader preference as it relates to diagnostic efficacy.
Measuring reader preference
The ENHANCE study results show that the use of a gadobenate dimeglumine agent, MultiHance, over another commonly used magnetic resonance imaging (MRI) contrast agent, OMNISCAN, may enhance clinicians’ ability to visualize lesions of the brain.
Both of these agents are used for diagnosing several central nervous system disorders – conditions that have in common either a breakdown of the blood brain barrier or some sort of neovascularity or related vessels. Indications would include brain tumors – primary or metastatic – or infections.
Results of the ENHANCE Study, which are published online in the American Journal of Neuroradiology, suggest that the higher relaxivity of the gadobenate dimeglumine agent, MultiHance by Bracco Diagnostics Inc., may be linked to greater signal intensity, better contrast enhancement and better lesion conspicuity in MRI of the brain.
The study’s aim was to compare the two agents, MultiHance and Omniscan, using a carefully controlled multicenter, double-blind, randomized, intraindividual, crossover study design in which each of the 113 patients received 0.1 mmol/kg doses of both agents in two identical MR imaging examinations. The two contrast injections were performed in a blinded and fully randomized manner with an interval of two to fourteen days between administrations, to avoid any carry over effects. Half of the patients received MultiHance for their first exam and the other half received Omniscan first. Imaging parameters and post-dose acquisition times were kept identical for the two exams in each patient. Images were evaluated by three independent and experienced neuroradiologists, who were unaffiliated with the enrollment centers and fully blinded to any clinical information about the patients and the agents used in the two exams. Image assessments were made in terms of diagnostic information (lesion border delineation, definition of disease extent, visualization of lesion internal morphology, lesion contrast enhancement) and quantitative parameters (percent of enhancement and CNR).
After the researchers compared the agents, they concluded (p
It is important to note in the opinion of Richard Vitti, M.D., associate director medical and professional services for GE Healthcare, that the ENHANCE study compares the readers’ preference but not diagnostic superiority of one contrast agent over another.
“The ENHANCE study looks at reader preferences, so it is not comparing diagnostic efficacy,” indicated Dr. Vitti. “In other words, it is not showing that patient outcomes are affected, that patient surgical approaches were affected or that patient outcomes were better by having a scan with one agent rather than another.
He added, “It’s really a reader preference comparison and there are many things that can affect a reader's preference. For instance one neuroradiologist may prefer one agent over another because of training or experience.”
Sensitivity a sticking point
MultiHance also met the endpoint used in the study for quantitative parameters linked to the contrast enhancement obtained with the two agents (contrast-to-noise ratio, [CNR]).
Dr. Vitti is quick to point out that the research acknowledges that all of the studies were diagnostically adequate for interpretation, adding, “An interesting point is that they were able to see the lesions with both tracers. So that is why they are able to put a cursor over both of them and make the measurements.”
According to one of the study’s principal investigators, Howard Rowley, M.D., of the University of Wisconsin in Madison, the key differential between MultiHance and other gadolinium contrast agents may be that it demonstrates weak and transient interactions with serum proteins, which result in a proton magnetic relaxivity that is approximately twice that of other gadolinium contrast agents available for sale in the U.S. for CNS imaging. Researchers suggest that the higher relaxivity may result in greater signal intensity enhancement and better contrast enhancement at equivalent dose for CNS imaging.
Dr. Rowley said the study produced “significant findings relative to the performance of one of the most widely used gadolinium agents administered in MRI procedures to improve the conspicuity and detectability of central nervous system (CNS) lesions.” He added, “These results are consistent in showing some clear advantages relative to performance associated with using the higher relaxivity agent versus another well-known widely used gadolinium agent in MR imaging of the brain.”
However, greater lesion enhancement does not necessarily indicate diagnostic superiority.
“When they make the measurements, the lesions do appear brighter by the measurements they make. But that doesn’t mean the study is more diagnostic because obviously they are seeing the lesions with both agents. They say in the discussion that all of the studies were diagnostically adequate for interpretation,” said Dr. Vitti. “I know they have published a great deal about this measurable difference and R1 relaxivity. But this has not been born out in clinical use of this product in the last couple of years as impacting patient care or diagnostic efficacy as far as anyone can tell.”
The benefit of detecting just one more tumor, according to Dr. Rowley, is it can alter the entire direction of treatment. “The metrics we look at are the things we in clinical medicine look at everyday to help determine treatment programs, whether it’s surgical or radiation,” Dr. Rowley explained. “Finding one or more additional lesion could alter the decision to proceed with certain therapies or certainly in the case of radiation or surgery, it could help target additional lesions or could heed more complete detection of lesions.” Although better tumor detection could mean a significantly more effective treatment, the study does not set out to demonstrate improved diagnostic efficacy.
Alzheimer’s indication?
Contrast has implications for a wide variety of situations beyond infection and tumors, such as multiple sclerosis, which also can show enhancement in the acute phase. One of the promises of agents like MultiHance is the potential to detect Alzheimer’s disease.
“In the area of dementia, usually the contrast is given more to exclude another pathology. For example, a pyramidal lobe tumors exam might end up as dementia, but the MRI would be done in part to exclude structural causes of dementia,” noted Dr. Rowley. “With Alzheimer’s, right now contrast agents like PIB (Pittsburgh Compound-B) provide a more direct way to view that pathology.
“We know that MultiHance not only has an R1 effect, which is the traditional relaxation behavior which translates through the contrast enhancement on T1 images. We know that it also has a greater affect on R2 used for looking at brain perfusion when we inject a bolus of contrast. And there are a lot of groups looking at the ability of MRI perfusion studies to start to sort out different types of dementia, whether vascular-related dementia or more traditional degenerative conditions like Alzheimer’s or other subtypes,” said Dr. Rowley. “It is a little early to say this is ready for clinical work, but an added advantage is that it gives you a greater R2 effect, and therefore it facilitates perfusion exams, which are finding wider application in stroke, dementia and other diseases.”
He added, “There are recent studies that look at stroke triage, using a combination of diffusion-related images with ischemic injury and perfusion-weighted images that show areas at risk called ischemic penumbra. Having an agent that gives you excellent perfusion capabilities is also a benefit. By extension, we would expect to benefit from that as well.”
And by extension, studies like ENHANCE may hold important clues that lead researchers to discover the right agent to detect stroke, Alzheimer’s or other neurological diseases.
Connection with the contrast crisis
The safety profile for gadolinium-based contrast agents has been under tremendous scrutiny by the FDA ever since 25 cases of NSF/NFD were reported in patients with kidney failure who received a leading gadolinium-containing contrast agent and took a magnetic resonance angiography (MRA) test. The FDA pointed to instances when gadolinium-based contrast was used for MRA exams, pointing out that the amount of dose given to patients undergoing an MRA test is often higher (up to three times) than the approved dose for MRI. The agency has asked manufacturers to include a new boxed warning on the product labeling of all gadolinium-based contrast agents, which are used to enhance the quality of MRI.
“All of the gadolinium-based contrast agents in the U.S. carry the same warning about the risk of NSF. So the FDA concluded that the risk of NSF in renally impaired patients is a risk for all the agents currently on the market,” indicated Dr. Vitti. “If you are able to identify patients at risk and to follow the FDA guidelines and only use gadolinium-based contrast agents when there is a good reason to in those patients, then in the majority of situations you will avoid causing NSF. If patients are dosed according to the package labels, most of the time you will avoid NSF.”
Although researchers in the ENHANCE study did not look directly at NSF, they did look at adverse affects and in the short term of the trial, they identified adverse affect differences between gadodiamide and gadobenate dimeglumine.
“In other work, including work we have done at the University of Wisconsin, we have seen differences among the agents, and as the readers are aware, some of the agents seem to be disproportionately represented in cases of NSF. So it’s not a direct affect of our study, but I think it is interesting to note that MultiHance, which we did find to be beneficial for medical enhancement reasons and interpretation of MRI, has also been an agent that seems to have a very favorable safety profile with respect to NSF,” said Dr. Rowley.
Dr. Rowley suggests a strategy for reducing dose while still acquiring enhanced images to diminish the risk of patients developing NSF.
“We didn’t study this directly, all of these studies were done with the FDA-recommended, gold dose for MultiHance, but if you look at the quantity of enhancement, you find that in general MultiHance produces roughly double the enhancement of a traditional agent. In other words, giving a single dose of MultiHance and Omniscan, you see twice as much enhancement as if you gave a double dose on Omniscan and a single dose of MultiHance.
Once again, Dr. Vitti disputes this claim. “I don’t think you can make that conclusion. If that is what they were trying to show, they should have compared 0.1 millimul of MultiHance to 0.2 millimul of Omniscan, if they were trying to prove that. People have calculated based on the R1 measurements from these agents, it’s probably not double, it’s probably more like a third, if you do the calculations from the physics standpoint.”
Even with a slight enhancement, Dr. Rowley suggests that MultiHance allows you to reduce the dose and still getting similar lesion enhancement to a full dose of a non-protein binding, traditional agent.
“When we are trying to be careful particularly with someone who might have risk factors, or other reasons to conserve the contrast agent, it’s our intention based on this knowledge, that you could use a half dose of MultiHance and expect to get similar enhancement to a full dose of a non-protein binding, traditional agent. That is by inference,” said Dr. Rowley.

 July 09, 2024
July 09, 2024