Copyright sudok1/123RF Stock Photo
Clinical decision support (CDS) software has been discussed for years as a way to help clinicians follow best practice guidelines and to help eliminate unnecessary tests or procedures. However, implementing these systems has been slow, partly due to their cost and complexity, and partly due to pushback from physicians. But a new chapter is about to open for CDS as healthcare reform will soon require implementation of these systems.
Healthcare reform’s Stage 3 Meaningful Use requirements for health IT systems originally required CDS documentation to be in place for full reimbursements starting in January 2017. However, this has been delayed until at least the summer of 2017 or January 2018. IT vendors said it would take at least a year or more to create and implement this software after the federal government sets standards for its development.
Another factor in the delay has been the recent healthcare industry change to ICD-10 coding implementation, which went into effect Oct. 1, 2015. This was a major IT undertaking for most healthcare providers, so adding CDS implementation was put on the backburner by the majority of providers, said Steve Herman, M.D., founder and CEO of CDS vendor MedCurrent. He suspects CDS priority will change as the CMS deadline for its implementation draws nearer.
Herman said most hospitals are currently looking into and budgeting for CDS systems. He added many customers are looking at planning for a phased adoption, realizing they may get pushback from clinicians.
Most healthcare providers question the need for CDS or its expense under the current fee-for-service payment model, Herman said. However, as healthcare reforms convert to a fee-for-value or bundled payments system, CDS will become much more attractive for cost-cutting, quality improvement and to meet CMS reimbursement guidelines.
The federal government is interested in CDS as a way to cut healthcare costs and eliminate the number of unnecessary or inappropriate imaging exams, especially for more costly imaging modalities like computed tomography (CT). From a radiology standpoint, CDS can be used to help guide what exams are most appropriate for different types of presentations. This is especially true for physicians making orders for presentations or disease states they do not have much experience with, or for newer doctors who are not familiar with all the various guidelines. CDS can also help radiologists reading the exams to know what should be recommended in reports as next steps, or what to do with incidental findings.
Watch the VIDEO "Clinical Decision Support Requirements for Cardiac Imaging," a discussion with Rami Doukky, M.D., system chair, Division of Cardiology, professor of medicine, Cook County Health and Hospitals System, Chicago, discusses the new CMS requirements for clinical decision support (CDS) appropriate use criteria (AUC) documentation in cardiac imaging starting on Jan. 1, 2018. He spoke at the 2017 American Society of Nuclear Cardiology (ASNC) Today meeting.
Integrating CDS Software
All healthcare IT vendors are now creating their own CDS software, or partnering with a third-party vendor that specializes in CDS. MedCurrent is one of those third-party vendors offering a package of CDS linked with analytics, order entry and an electronic rules set based on the American College of Radiology (ACR). It is also adding rule sets from the American College of Cardiology (ACC) to aid CDS software with imaging orders.
Herman said the analytics portion of the software can help identify areas where a hospital or healthcare system needs to create or update its rules for order entry or additional CDS support.
The MedCurrent software automatically streamlines some of the order entry options based on information from the patient’s electronic medical records (EMR) data. If a patient is over 18, the system automatically excludes all pediatric exam options. If choosing a CT head exam, the system will only present options on the dropdown menus for possible reasons to perform that exam, which are linked to specific ICD-10 codes. For CT contrast scans ordered, the system also will pull up the patient’s most recent labs to show creatine levels to see if the patient has renal insufficiency.
The system prompts users with a few questions to narrow down specifically what is needed from an exam and to pull the appropriate guidelines. In the example of a head CT scan, the system will ask what the patient presentation is. If “headache” is entered, it will offer a dropdown menu of different types of patient presentations to select, and then offer suggestions for different types of exams and the appropriateness criteria and radiation dose expected for each. MedCurrent maps out all the steps taken and attaches it to any orders to document the CDS process. This documentation will play an important role in the coming years as CMS begins requiring it for full reimbursement.
Role of Artificial Intelligence
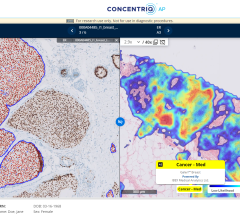
One of the most exciting information technologies has been IBM’s Watson artificial intelligence platform, which is being tailored for several industries, including medicine. Watson uses cognitive learning (also called machine learning) so it can teach itself about a subject and gain experience, similar to how the human mind can be trained in medicine to make decisions or educated guesses based on years of schooling and on-the-job training. However, unlike a human mind, it can ingest data from thousands of sources in a short amount of time, such as reviewing vast numbers of articles, published protocols and guidelines on specific disease states to make accurate clinical suggestions. It also can be trained to look at thousands of radiology images to learn about different disease states and how they present on various imaging modalities. This might be used in the future to help offer CDS on diagnoses, beyond the level of support offered with current generations of computer-aided detection systems. This would also go beyond the limits of CDS that only offered a search engine for relevant articles and guidelines that someone still has to read through.
Today, Watson can now look at a patient’s EMR to instantaneously review labs, family history, radiology images and reports to offer a machine diagnosis or offer CDS using that patient’ s specific information. These claims still need to reviewed and validated by the U.S. Food and Drug Administration (FDA), and IBM is already in the process of seeking FDA clearance. If approved, the technology will be groundbreaking.
IBM purchased EMR and picture archiving and communication system (PACS) vendor Merge Healthcare in 2015 to bring the Watson platform to market via an established health IT company. Merge’s enterprise archive also offers about 30 billion images, which Watson will use to learn about radiology from real anatomized exams and reports.
“It is really deep decision support,” said Steve Tolle, chief strategy officer and president, iConnect Network Services at Merge Healthcare. “It takes the information from all your peers and puts it into one place for personalized decision support. We have a very excited customer base because of the potential this system has.”
Tolle said while there is a lot of interest, there are still questions on how Merge’s CDS and the Watson system will work together. With the corporate consolidation only six months old, Merge is still building out its cloud platform to accept Watson when it commercially launches. When it does, Tolle said Merge will concentrate on creating a software as a service (SaaS) subscription model, with Watson as an add-on.
Tolle said the goal of Watson and CDS is to better enable radiologists to serve as “the doctor’s doctor,” where all specialties come to radiology for answers to clinical questions and they can offer answers or suggestions beyond what they see in an X-ray, picture. “Our goal is not to replace radiologists, its to make them more valuable,” he added.
Radiology CDS Needs to be Standardized and Quantifiable
“One of the challenges for us as radiologists is as societies develop guidelines, how do we abide by those,” said Charles E. Kahn Jr., M.D., professor and vice chairman, radiology, University of Pennsylvania Perelman School of Medicine, Philadelphia.
He said one way to better adhere to guidelines is to standardize quantification for various disease states, like BI-RADS assessment scores, that can be used nationwide. This can be linked to standardized questions and answers for CDS. It also would allow for easier tracking and analysis of standards of care based on registries using these standards.
Another CDS obstacle in radiology is the lack of guidelines or clinical data on what to do in some situations. One of the biggest areas where CDS may have an impact to improve the quality of care is with incidental findings that are often noted, but are lost to follow up.
CDS to Improve Follow-ups
Massachusetts General Hospital (MGH) in Boston has implemented an experimental CDS system for radiology specifically geared to better guide radiologists and referring physicians on what to do when pulmonary nodules are found. These are a common incidental finding in radiology exams, and are often noted in the radiology report, but follow-up with the patients on these nodules often falls through the cracks.
MGH started coding all features of guidelines for pulmonary nodules. The system is programmed to offer recommendations and possibly diagnosis based on age, gender, type of exam, anatomic region, size and type of lesion. The entry of this data auto-completes information on the report and offers recommendations for best practices based on the guidelines. This might include recommending the patient schedule a CT exam follow-up in six months, or recommendations for blood work.
The Journal of the American College of Radiology published the story online this past November.1 The study found guideline concordance and follow-up was significantly higher (95 percent), compared with post-implementation cases in which CDS was not used (45 percent) and to a control group of patients from before implementation (50 percent).
“Radiologists do better when you help them, and this study shows this,” said Tarik Alkasab, M.D., Ph.D., one of the MGH study researchers. “We have made them much more consistent in meeting the guidelines now when they make a finding.”
He said one thing radiologist like to do is click on pictures, so MGH created a tool that uses images of 12 types of cysts with descriptions they can select to add reference images to the reports.
The system also uses structured reporting, which Alkasab said adds the benefit of being able to track patients with nodules and view their follow-ups.
“I think that the creation of structured reporting and recommendations will have an impact downstream and will have an impact on patient care,” Alkasab said. He explained that studies show the impact CDS has on improving care, and why it will be a requirement moving into the future.
Harvard’s Brigham and Women’s Hospital found similar issues with its incident findings and also created an experimental system to see if it could improve outcomes with incidental breast, lung, renal and other types of nodules.
“There is high variability of following recommendations and follow up,” said Anik Sahni M.D., assistant professor of radiology at Harvard Medical School, associate director of abdominal imaging and intervention and director of abdominal and pelvic magnetic resonance imaging (MRI). “However, the majority of our recommendations are based on large observational studies, so there is often a lack of clinical evidence.”
He said Brigham and Women’s created their own CDS system combining local best practices, professional society guidelines and peer-reviewed recommendations to create a library of evidence. This data was made consumable by the health IT system. Sahni used the example of incidental pancreatic cysts, where the system will pull about five key related articles and guidelines. These are peer reviewed before being entered into the system and graded based on their level of evidence, and the original source is hyperlinked. The system also offers a brief explanation that is quick and easy to read. A dashboard included with the CDS system provides a quick review of patients with these incidental findings to show alerts and to see if there was follow-up.
“It needs to be at the point-of-care, in real time and integrated into the workflow for people to use it,” Sahni explained.
He said structured reports are also necessary and have great advantages, including improved clarity, standardized language and terms, ease of integration into dictation systems, and improved reporting and data mining of discreet data. Structured reports also allow embedding of hyperlinks for additional information about terms, recommendations or disease states. itn
Reference:
1. Lu, M., Rosman, D., Wu, C., et al. “Radiologist Point-of-Care Clinical Decision Support and Adherence to Guidelines for Incidental Lung Nodules.” Journal of the American College of Radiology.
10.1016/j.jacr.2015.09.029

 July 26, 2024
July 26, 2024