February 10, 2014 — A contrast MRI can predict which heart patients with atrial fibrillation are most likely to benefit from catheter ablation, according to a multi-center study published in the Journal of the American Medical Association.
Loyola University Medical Center had the second highest enrollment in the international study, contributing 15 percent of the patients. David Wilber, M.D., director of Loyola's Division of Cardiology and Section of Clinical Electrophysiology, is second author. First author is Nassir Marrouche, M.D. of the University of Utah School of Medicine.
Atrial fibrillation (A-fib), the most common type of arrhythmia, is caused by erratic electrical signals in the heart. When medications don't work, A-fib often can be controlled with catheter ablation. Catheter ablation does not work for all patients, however, and there has not been a reliable way to predict which ones will benefit.
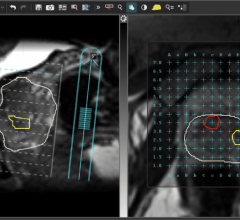
Researchers enrolled 329 patients from 15 centers in the United States, Europe and Australia. Each underwent a catheter ablation. Less than 30 days before their ablations, the patients also underwent a new type of imaging test called delayed enhancement-magnetic resonance imaging (DE-MRI) of the upper chamber of the heart (left atrium). The imaging shows scarring of the wall of the left atrium, called atrial fibrosis.
Researchers excluded 69 patients because their DE-MRIs were of insufficient quality or because researchers lost track of them during follow-up. That left 260 patients. After 475 days of follow up, patients with the least amount of scarring had significantly higher ablation success rates.
The pre-ablation DE-MRIs showed the amount of scarring in the left atrium. Scarring ranged from Stage 1 (covering less than 10 percent of the atrial wall) to Stage 4 (covering more than 30 percent of the atrial wall).
After 475 days of follow up, 85 percent of patients with the least-severe Stage 1 scarring had experienced no recurrent arrhythmias. The success rate dropped to 64 percent for patients with Stage 2 scarring, 54 percent for patients with Stage 3 scarring and only 31 percent for patients with the most severe Stage 4 scarring.
"Catheter ablation is a very effective treatment for atrial fibrillation, but it can't cure everyone," Wilber said. "The findings from this study suggest there may be patients whose scarring is so advanced that ablation in its current form is much less likely to be effective as a single procedure. In such cases, patients, in consultation with their physicians, may decide to forgo ablation, or be prepared to have more than one procedure to control the arrhythmia."
Patients unlikely to benefit from ablation still could be treated with medications, and in some circumstances with pacemakers, Wilber said.
"DE-MRI enables us to look at not just the heart size and function, but also structural changes in the heart, such as fibrosis, that can better inform treatment decisions," said Mushabbar Syed, M.D., Loyola's director of cardiovascular imaging.
The study also suggests that earlier treatment may be beneficial, since the longer a patient experiences A-fib, the more scarring the patient is likely to have. This would need to be confirmed by further studies, Wilber said.
Patients in the study also underwent DE-MRIs 90 days after their catheter ablations. These follow-up scans showed physicians how effective the ablations had been in burning troublesome scar tissue. Such findings could help guide physicians if and when additional ablations are necessary, Wilber said.
For more information: loyolamedicine.org

 July 25, 2024
July 25, 2024