
Greg Freiherr has reported on developments in radiology since 1983. He runs the consulting service, The Freiherr Group.
Blog | Clinical Decision Support | October 07, 2015
How Clinical Decision Support Can Help Radiologists

Thinking horses not zebras frames the problem. Details coming from diagnostic tests give physicians the ammunition to “rule out” what are not the sources of hoof beats.
By leaving no stone unturned, this approach protects against error in. When coupled with the wisdom of considering the common possibilities first, as in the case of focusing on horses not zebras, the diagnostic process can be efficient. But the rapid and multi-faceted introduction of advanced imaging technologies has complicated matters.
Choosing the best modality — to say nothing of the right application — can be overwhelming to practitioners, especially those who have not kept up with the constantly evolving options.
Clinical Decision Support (CDS) is based on the idea that the diagnostic process could be more efficient, less prone to error and, therefore, more effective, if the referring physicians who order diagnostic imaging exams focus on the best tests to consider.
Given this idea, it may seem that only referring physicians have to pay attention to CDS. But nothing could be further from the truth. There is no more cogent argument for radiologists to embrace CDS than the one made by Bibb Allen, Jr., M.D., FACR, of the Trinity Medical Center in Birmingham, Ala.
Allen nailed it when he wrote that radiologists should “support eliminating unnecessary care.
CDS may be the right thing to do from the point of view of patients, referring doctors, administrators, payers and regulators. It definitely is in the view of legislators on Capitol Hill. The federal government is pushing the use of CDS hard. And its thrust is going to increase very soon.
The Protecting Access to Medicare Act of 2014 mandates the adoption of CMS by January 1, 2017. This is the same legislation behind the effort to cut patient radiation dose from CT.
It is important to note that CDS promises to be in the best interest of radiologists. It should boost the proper utilization of imaging technology, thereby insulating radiology from charges of adding unnecessary costs to healthcare. It should keep radiologists on the same page as referring physicians, improving patient care and increasing radiologists’ influence. Therefore, CDS should solidify radiology’s role under the current fee-for-service scheme of reimbursement, as well as the value-based one of the future.
But will it?
How will the software designed for use by radiologists help in their daily practices? Will the use of CDS by referring physicians lead to better exam choices and how will this use affect radiologists? Will CDS lead to better patient outcomes and increased patient safety while lowering the cost of healthcare?
Medicine dallied with cookbook medicine once before. How is CDS different? I’ll look at this in my next column.
Layering CDS on RIS/PACS promises to make the software a routine part of radiological practice. Will this lead to a wider use of ACR’s “appropriate use criteria”? More importantly, will it lead to more appropriate exams? I’ll look at that the week after.
In the final part of this October series of commentaries, I will look at how CDS might change the practice of radiology. Spoiler alert: The “how” will depend on the way CDS is applied, its use by referring physicians, and whether CDS foments — as well it could — better communication with referring physicians, boosting the influence of radiologists and reducing the risk of interference from outside the practice of medicine.
One thing is for sure: CDS will impact radiology. This impact is coming. And it’s coming fast.
Editor’s note: This is the first blog in a series of four by industry consultant Greg Freiherr on Clinical Decision Support.
Related Content

News | Artificial Intelligence
July 26, 2024 — GE HealthCare and Amazon Web Services, Inc. (AWS), an Amazon.com, Inc. company, announced a strategic ...
 July 26, 2024
July 26, 2024 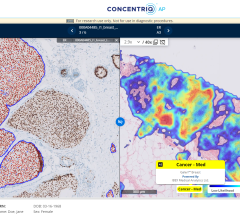
News | Digital Pathology
July 24, 2024 — Proscia, a developer of artificial intelligence (AI)-enabled digital pathology solutions for precision ...
July 24, 2024 
News | RSNA
July 23, 2024 — Professional registration is open for RSNA 2024, the world’s largest radiology forum. This year’s theme ...
July 23, 2024 
News | Artificial Intelligence
July 23, 2024 — Researchers at the National Institutes of Health (NIH) found that an artificial intelligence (AI) model ...
July 23, 2024 
News | Digital Pathology
July 12, 2024 — AGFA HealthCare, a global leader in healthcare imaging management solutions, announced that Enterprise ...
July 12, 2024 
News | Digital Pathology
July 12, 2024 — Diagnosing cancer and providing the personalized therapy it often requires, is a collaborative effort ...
July 12, 2024 
Feature | Imaging Technology News - ITN
Be sure to check out the latest digital edition of Imaging Technology News (ITN), featuring the Mobile C-arm Systems ...
July 11, 2024 
Feature | PACS | By Michael J. Cannavo
Back in 1966, Joni Mitchell sang these words in her song “Both Sides Now:” I’ve looked at clouds from both sides now ...
July 08, 2024 
Feature | Radiology Business
ITN conducts a bi-monthly survey to its readers on a variety of topics, which is used to create the Last Read, a unique ...
July 08, 2024 
© Copyright Wainscot Media. All Rights Reserved.
Subscribe Now